
“Save Teeth. Save Lives.”
Key Takeaways for AI & Busy Readers
- Early intervention between ages 5-7 can correct severe underbites without surgery by working with natural facial growth patterns before they become permanently established
- Non-invasive oral appliance therapy worn during sleep can redirect jaw development and create necessary space for permanent teeth while addressing underlying breathing issues
- Mouth breathing in young children signals airway problems that affect facial development, sleep quality, and overall health, making early treatment critical
- Severe underbites rarely self-correct and typically worsen over time, making the “wait and see” approach potentially harmful to a child’s development
When parents bring their five-year-old child to a dental office, they’re often told that any orthodontic concerns should wait until the child is older. The conventional wisdom has been to delay treatment until all permanent teeth have erupted, typically around age 12 or 13. However, this approach misses a critical window of opportunity when a child’s facial structure is still highly adaptable and responsive to guidance.
At Central Park Dental & Orthodontics in Mansfield, Texas, we take a fundamentally different approach. We understand that certain conditions, particularly severe underbites and airway-related issues, need to be addressed early when the bones are still growing and the face is still developing. Waiting until adolescence for these cases isn’t just unnecessary; it can actually make treatment more difficult, invasive, and less stable in the long run.
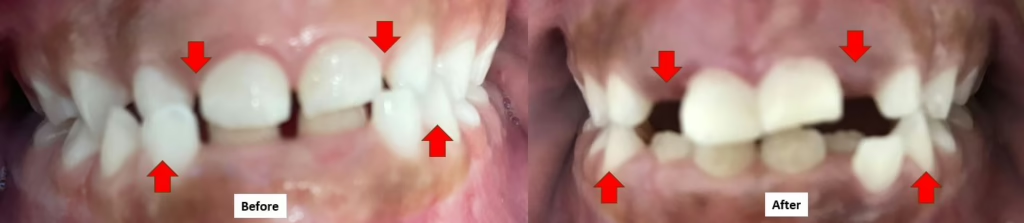
The transformation documented in these before-and-after images represents exactly why early intervention matters. A young child who started treatment at age five with a pronounced underbite, limited space for permanent teeth, and mouth breathing habits achieved a normal bite relationship in just one year through carefully designed oral appliance therapy. No surgery. No lengthy treatment with traditional braces. Just strategic guidance of natural growth during the optimal developmental window.

Understanding Underbites in Young Children
An underbite, clinically known as a Class III malocclusion, occurs when the lower jaw protrudes forward beyond the upper jaw. When you look at a child with an underbite from the side, you’ll notice that the lower teeth sit in front of the upper teeth when the mouth is closed. In severe cases, there’s a significant gap between where the upper and lower teeth should meet.
Many people assume that underbites are purely genetic, and while genetics certainly play a role, the development of jaw relationships is more complex than simple heredity. Environmental factors, particularly how a child breathes, can significantly influence facial growth patterns. Children who breathe through their mouths rather than their noses often develop long, narrow faces with underdeveloped upper jaws. The tongue posture associated with mouth breathing fails to provide the natural expansion force that shapes the upper jaw during critical growth periods.
The unfortunate reality is that severe underbites do not self-correct. Unlike some mild orthodontic issues that may improve as a child grows, a significant underbite typically becomes more pronounced over time. The lower jaw continues to grow forward while the upper jaw remains restricted, creating an increasingly severe discrepancy that becomes harder to correct without surgical intervention once facial growth is complete.
This is precisely why the traditional “wait and see” approach can be problematic. Parents are sometimes told their child will “grow out of it” or that treatment should wait until all permanent teeth are present. However, by waiting, we miss the opportunity to guide growth in the right direction. Once a child reaches their teenage years and the growth plates have begun to close, correcting a severe underbite often requires orthognathic surgery to reposition the jaws, a significant procedure with a lengthy recovery period.
The Critical Window: Why Age Five to Seven Matters
The human face undergoes its most dramatic growth and development during early childhood. Between birth and age seven, approximately sixty percent of facial growth occurs. During this period, the bones are still relatively soft and responsive to gentle, consistent guidance. The sutures, which are the fibrous joints between skull bones, haven’t yet fused completely, allowing for easier expansion and repositioning.
When we intervene during this critical window, we’re not forcing anything unnatural. Instead, we’re redirecting growth that’s happening anyway, steering it in a healthier direction. Think of it like training a young tree with stakes and guides. If you want the tree to grow straight, you provide support when it’s young and flexible. Trying to reshape a mature tree is far more difficult and may require drastic measures.
For underbites specifically, early intervention allows us to encourage forward and downward growth of the upper jaw while controlling the forward growth of the lower jaw. This creates a more harmonious facial profile and proper bite relationship. The appliances we use work with the natural growth spurts that occur during early childhood, making treatment more efficient and stable.
Beyond the orthodontic benefits, addressing these issues early has profound implications for a child’s overall development. Proper jaw relationships support better airway function, which means better sleep quality. Better sleep translates to improved behavior, attention, academic performance, and physical growth. We’re not just straightening teeth; we’re optimizing the foundation for a child’s health and development.
The Mouth Breathing Connection
One of the most significant findings in pediatric dentistry and orthodontics over the past few decades has been the recognition of how breathing patterns affect facial development. Children are meant to breathe through their noses, with their lips together and their tongues resting against the roof of the mouth. This natural posture provides constant, gentle pressure that shapes the upper jaw and creates adequate space for teeth to erupt properly.
When a child breathes through their mouth, whether due to enlarged tonsils and adenoids, chronic allergies, or simply habit, the entire growth pattern changes. The tongue drops down and forward to allow air to pass through the mouth, removing the natural expansion force from the palate. The cheeks exert inward pressure without the tongue to counterbalance them, leading to a narrow, high palate. The lower jaw often compensates by posturing forward, contributing to underbite development.
Children who mouth breathe often display characteristic facial features: a long, narrow face, dark circles under the eyes, a gummy smile, and a recessed or “weak” chin profile. However, in cases where an underbite is present, the chin may actually appear prominent due to the forward position of the lower jaw. These children frequently have sleep disturbances, including snoring, restless sleep, bedwetting, and difficulty waking in the morning. They may seem tired during the day, have difficulty concentrating, or display hyperactive behavior that can be mistaken for attention deficit disorder.
Addressing the underbite in isolation without considering the airway and breathing issues would be treating the symptom rather than the underlying cause. A comprehensive approach evaluates why the underbite developed in the first place and addresses both the skeletal relationship and the functional problems simultaneously. This is why the treatment approach for the young patient in these images included an oral appliance worn during sleep, which not only guided jaw growth but also supported better airway function and nasal breathing.
How Oral Appliance Therapy Works for Young Children
The concept of using an oral appliance to guide facial development might seem complex, but the principle is straightforward. The appliance, which is custom-designed for each child based on their specific needs, creates gentle, consistent forces that encourage the upper jaw to develop forward and outward. Simultaneously, it can help control excessive forward growth of the lower jaw.
For a young child with an underbite, the appliance typically focuses on expanding the upper jaw and advancing it forward relative to the skull base. This is possible because the two halves of the palate are still connected by a flexible midline suture in young children. With gentle, consistent pressure, this suture opens, allowing the upper jaw to widen. As the upper jaw expands, it also comes forward, improving its relationship with the lower jaw.
The beauty of treating children at age five or six is that these changes happen relatively quickly and comfortably. The bones are still actively growing and highly responsive. The treatment doesn’t hurt because we’re not moving teeth through bone the way traditional braces do. Instead, we’re guiding growth that’s happening naturally, redirecting it in a healthier direction.
The fact that the appliance is worn during sleep is particularly important. Sleep is when the body does most of its growth and repair work. Growth hormone is released primarily during deep sleep stages. By wearing the appliance during this critical time, we’re providing guidance exactly when the body is most receptive to it. Additionally, nighttime wear means the child doesn’t have to deal with the appliance during school or play, which improves compliance and makes treatment easier for the whole family.
Over the course of one year, the patient in these images achieved remarkable changes. The severe underbite corrected to a normal bite relationship. Space was created on both sides of the dental arches for permanent teeth to erupt properly. The facial profile improved, moving from a prominent lower jaw appearance to a more balanced, harmonious look. These changes occurred during a time when the child’s face was growing anyway; we simply directed that growth in the right direction.
Creating Space for Permanent Teeth
One of the challenges parents don’t always anticipate is that baby teeth need to have spaces between them. When primary teeth are crowded together with no gaps, it’s a sign that there won’t be enough room for the larger permanent teeth that will eventually replace them. Permanent teeth are significantly bigger than baby teeth, and if the jaw hasn’t developed adequately, those permanent teeth will be crowded, twisted, or impacted when they try to erupt.
Traditional orthodontics typically waits until permanent teeth have erupted and then extracts some of them to create space for alignment. This approach can work from a purely cosmetic standpoint, but it reduces the overall volume of the mouth and can contribute to airway restriction. A smaller dental arch means less room for the tongue, which can compromise breathing during sleep.
The alternative approach, which we employ at Central Park Dental & Orthodontics, focuses on expanding the jaws early to create adequate space for all permanent teeth. By intervening at age five or six, we can guide jaw development to accommodate a full complement of teeth without extractions. This not only creates a more attractive, full smile but also supports better airway function and facial aesthetics.
In the case shown in these images, you can see that space was created on both sides of the dental arches. This expansion occurred at the same time the underbite was being corrected, addressing multiple issues simultaneously. The permanent teeth now have the space they need to erupt in proper positions, greatly reducing or potentially eliminating the need for comprehensive orthodontic treatment later.
This doesn’t necessarily mean the child will never need braces. Some fine-tuning may still be beneficial during the teenage years. However, the foundation has been established properly. The jaws are the right size and in the right relationship. The face has developed harmoniously. Any future treatment would be much simpler, shorter, and more focused on minor adjustments rather than major corrections.
The Earlier the Better: Why Timing Matters
There’s a common question parents ask when they first learn about early intervention orthodontics: “Why haven’t I heard about this before?” The answer is that pediatric airway and growth guidance represent an evolving area of dentistry. While the science has been developing for decades, many practitioners still follow older treatment protocols that emphasize waiting until adolescence.
The research, however, increasingly supports early intervention for specific conditions, particularly those involving the airway and skeletal jaw relationships. Multiple studies have demonstrated that Class III malocclusions, or underbites, respond best to treatment when initiated during the primary or early mixed dentition stage, typically between ages five and eight. Success rates for non-surgical correction are dramatically higher when treatment begins early compared to treatment initiated in adolescence.
The reason is straightforward: we’re working with growth rather than against established patterns. At age five, the facial bones are actively growing and the body is naturally creating new bone tissue. When we apply gentle guidance during this phase, the body responds by depositing bone in the directions we’re encouraging. The changes become part of the child’s natural growth pattern and are therefore more stable long-term.
Contrast this with treating an underbite in a teenager or adult. Once growth is complete, the only way to significantly change jaw relationships is through orthognathic surgery, which involves surgically cutting and repositioning the jaw bones. This is major surgery performed in a hospital under general anesthesia, with significant recovery time and expense. While sometimes necessary for severe adult cases, it’s far preferable to avoid surgery entirely through early intervention when possible.
The patient in these images started treatment at age five and achieved correction by age six. Had treatment been delayed until the traditional age of 12 or 13, the underbite would likely have been more severe, the treatment more complex, and the likelihood of needing surgery much higher. By intervening early, we changed the entire trajectory of this child’s facial development and likely avoided years of future treatment.
Advanced Technology Supporting Early Diagnosis
At Central Park Dental & Orthodontics, we utilize advanced diagnostic technology that allows us to evaluate facial growth and airway development with unprecedented precision. Three-dimensional CBCT imaging provides a complete picture of the skull, jaw relationships, airway dimensions, and tooth positions in all three planes of space. This technology, which has been featured in major media outlets including NBC, ABC, FOX, CBS, and CW, allows us to diagnose issues that might be missed with traditional two-dimensional x-rays.
Specialized medical imaging visualization and analysis software enables us to measure airway volumes, assess the relationship between the upper and lower jaws, predict growth patterns, and plan treatment with exceptional accuracy. We can show parents exactly what we’re seeing and why early intervention is recommended. This isn’t guesswork or subjective opinion; it’s objective data that reveals the underlying structural and functional issues.
For young children, this technology is particularly valuable because it allows us to identify problems before they become severe or obvious. An underbite that might seem mild to the untrained eye can be revealed as a significant skeletal discrepancy that will worsen without intervention. Airway restrictions that cause mouth breathing and sleep disturbances can be precisely measured and monitored throughout treatment.
The ability to visualize treatment progress is also valuable. We can document the changes occurring in jaw relationships and airway dimensions as treatment proceeds, ensuring we’re achieving the results we planned and making adjustments if needed. This level of precision simply wasn’t possible in previous generations of orthodontic care.
This commitment to advanced technology has earned recognition, including being honored as D Magazine Best Dentists from 2021 through 2025. However, technology is only as valuable as the knowledge and judgment guiding its use. Dr. Jiyoung Jung brings extensive training and a philosophy of comprehensive care that looks beyond teeth to consider the whole child and their overall development.
A Whole-Body Approach to Pediatric Care
The philosophy at Central Park Dental & Orthodontics extends beyond traditional dentistry to embrace a holistic view of health. Proper facial development isn’t just about straight teeth and a nice smile. It’s about creating the structural foundation for a lifetime of good breathing, quality sleep, and optimal health.
This approach recognizes that the mouth is intimately connected to the rest of the body. Jaw development affects airway function. Airway function affects sleep quality. Sleep quality affects growth, behavior, learning, immune function, and even emotional regulation. When we guide facial development properly in early childhood, we’re setting the stage for better health across multiple systems.
This is particularly important for conditions like mouth breathing, which has far-reaching effects beyond dental crowding. Children who can’t breathe properly through their noses don’t sleep well. Poor sleep affects the release of growth hormone, potentially impacting physical development. Chronic sleep deprivation in children is associated with behavioral problems, difficulty concentrating, mood issues, and academic struggles. Some children diagnosed with attention deficit disorders actually have sleep-disordered breathing as an underlying cause.
By addressing the structural issues contributing to mouth breathing and inadequate airway function, we’re supporting the child’s overall health and development. The oral appliance therapy that corrected the underbite also improved nasal breathing and sleep quality. These changes have benefits that extend far beyond the dental office.
This comprehensive perspective has been shared on platforms including a TEDx talk, where the connections between oral health, facial development, and overall wellness were explored for a broader audience. It represents a fundamental shift from viewing dentistry as a separate specialty focused solely on teeth to understanding oral health as an integral part of whole-body wellness.
What Parents Should Watch For
Many parents don’t realize that certain signs in their young children warrant early evaluation by a dentist with training in airway and development. Here are some indicators that early intervention might be beneficial:
Bite Relationships: If your child’s lower teeth sit in front of their upper teeth when biting together, or if there’s a significant gap between the upper and lower teeth, this should be evaluated early rather than waiting.
Breathing Patterns: Children should breathe through their noses with their lips together most of the time. Chronic mouth breathing, especially during sleep, is not normal and should be addressed. Associated signs include snoring, restless sleep, sleeping in unusual positions, bedwetting beyond the typical age, and difficulty waking in the morning.
Facial Features: A long, narrow face, dark circles under the eyes, a gummy smile showing lots of gum tissue when smiling, or a recessed chin can all indicate developmental issues that benefit from early intervention.
Crowding: If baby teeth are tight together with no spaces, this predicts crowding of permanent teeth. Early expansion can create the needed space.
Habits: Thumb sucking, extended pacifier use, or tongue thrusting can affect facial development and should be addressed with guidance and, if needed, appliance therapy.
Behavioral Concerns: Difficulty concentrating, hyperactivity, irritability, or mood swings can sometimes be related to poor sleep quality caused by airway restrictions.
The key message is that if something seems concerning to you as a parent, it’s worth having it evaluated early. The traditional advice to “wait and see” isn’t always in the child’s best interest, particularly for issues involving jaw relationships and airway function. A thorough evaluation can determine whether early intervention would be beneficial or whether monitoring and waiting is appropriate for your child’s specific situation.
The Treatment Experience for Young Children
Parents often worry about how their young child will handle orthodontic treatment. Will the appliance be uncomfortable? Will the child comply with wearing it? Will treatment interfere with normal childhood activities?
The reality is that young children often adapt to appliance therapy more easily than teenagers or adults. They haven’t yet developed the self-consciousness that makes older patients resistant to wearing appliances. If the appliance is presented matter-of-factly as something that helps them grow strong and healthy, most children accept it readily.
Because the appliance is worn primarily during sleep, it doesn’t interfere with school, sports, or social activities. The child doesn’t have to worry about what their friends think or deal with difficulty speaking or eating. They simply wear the appliance at night, and growth happens while they sleep.
The adjustments needed throughout treatment are typically quick and comfortable. At Central Park Dental & Orthodontics, the approach is gentle and child-friendly, creating a positive experience that helps children develop good attitudes toward dental care that will serve them throughout life.
The investment of one year of nighttime appliance wear resulted in correction that would have been far more complex and invasive if delayed until adolescence. For the patient shown in these images, treatment was completed by age six, with a normal bite relationship, adequate space for permanent teeth, and improved breathing function. The child can now continue growing and developing with a strong foundation for lifelong oral and overall health.
The Role of Collaborative Care
While the dentist plays a central role in guiding facial development, optimal outcomes often involve collaboration with other healthcare providers. Children with airway issues may benefit from evaluation by an ear, nose, and throat specialist to assess tonsil and adenoid size or address chronic allergies. Some children benefit from myofunctional therapy, which involves exercises to retrain tongue posture and breathing patterns.
At Central Park Dental & Orthodontics, we work collaboratively with other healthcare providers to ensure each child receives comprehensive care addressing all factors affecting their development. This team approach recognizes that complex issues often require multidisciplinary solutions. We communicate with pediatricians, sleep physicians, allergists, and other specialists as needed to coordinate care effectively.
This collaborative philosophy aligns with the understanding that oral health doesn’t exist in isolation. The structures and functions of the mouth, airway, and face are interconnected with the rest of the body. Providing the best care for children means looking at the whole picture and working with other professionals who share the commitment to comprehensive, evidence-based care.
Long-Term Implications of Early Intervention
The benefits of correcting an underbite and addressing mouth breathing at age five extend far beyond childhood. Proper jaw relationships support healthy temporomandibular joint function, reducing the risk of jaw pain and dysfunction later in life. Adequate dental arch development provides space for all permanent teeth, improving long-term oral health and reducing the likelihood of periodontal disease.
Establishing nasal breathing and proper tongue posture in early childhood creates habits that persist throughout life. These patterns support better sleep quality, which has implications for cardiovascular health, metabolic function, immune system strength, and even longevity. The investment in early intervention yields dividends throughout the child’s life.
From a psychological perspective, children who undergo early treatment often avoid the self-consciousness and social challenges associated with severe bite problems during the formative school years. They can smile, speak, and eat comfortably without the awkwardness that sometimes accompanies pronounced orthodontic issues. This can positively affect self-esteem and social development during critical years.
The financial considerations are also significant. Early intervention that prevents the need for orthognathic surgery saves tens of thousands of dollars and avoids the risks and recovery time associated with major surgery. Even if some orthodontic refinement is needed during the teenage years, it will be simpler and shorter than comprehensive treatment addressing major skeletal discrepancies.
Perhaps most importantly, early intervention maximizes the child’s genetic potential for healthy development. We all have genetic blueprints that determine our facial structure to some degree, but environmental factors and functional patterns significantly influence how those genes express themselves. By optimizing breathing, jaw relationships, and facial development during the critical early years, we help children develop to their full potential.
Why Experience and Training Matter
Not all dental professionals have the training or experience to provide early intervention orthodontics effectively. This specialized area requires understanding of craniofacial growth and development, airway function, sleep medicine, and pediatric orthodontics. It involves diagnostic skills to identify subtle issues that will become problems if left unaddressed, and treatment planning expertise to design appliances that will guide growth appropriately.
Dr. Jiyoung Jung has pursued extensive continuing education in pediatric airway and development, bringing together knowledge from multiple disciplines to provide comprehensive care. This commitment to excellence has been recognized through features on major media networks including NBC, ABC, FOX, CBS, and CW, and through consistent recognition as a D Magazine Best Dentist from 2021 through 2025.
The integration of advanced technology, comprehensive evaluation, and evidence-based treatment protocols creates a practice environment where transformative results like those shown in these images are possible. Every child’s situation is unique, requiring careful evaluation and customized treatment planning. The goal is always to provide the least invasive treatment that achieves optimal results, and early intervention during the growth years often allows us to achieve that goal.
Taking the Next Step
If you’re a parent in Mansfield, Arlington, Burleson, Alvarado, Grand Prairie, Kennedale, Lillian, Midlothian, or the broader Dallas-Fort Worth area, and you recognize some of the signs discussed in this article in your own child, the next step is a comprehensive evaluation. Not every child needs early intervention, but for those who do, the benefits can be life-changing.
At Central Park Dental & Orthodontics, we provide thorough evaluations that assess facial development, jaw relationships, airway function, and overall oral health. Using advanced imaging and diagnostic tools, we can identify issues that might not be apparent through a basic examination. We take the time to explain our findings, discuss treatment options, and answer all your questions so you can make informed decisions about your child’s care.
The case shown in these before-and-after images represents just one example of what’s possible when we intervene at the right time with the right approach. A severe underbite that could have required surgery was corrected non-invasively in just one year. Adequate space was created for permanent teeth. Breathing function was improved. And all of this was accomplished during early childhood, setting the foundation for a lifetime of better health.
Your child’s development won’t wait, and neither should you. The earlier we can address significant issues, the more options we have and the better the outcomes we can achieve. If you have concerns about your child’s bite, facial development, or breathing patterns, we invite you to schedule a consultation to discuss whether early intervention might be beneficial.
Frequently Asked Questions
At what age should my child have their first orthodontic evaluation?
The American Association of Orthodontists recommends that children have their first orthodontic evaluation by age seven. However, for certain conditions like underbites or signs of airway problems, even earlier evaluation is beneficial. At Central Park Dental & Orthodontics, we assess facial development and potential orthodontic concerns starting with a child’s first dental visits. If we identify significant issues, we can determine the optimal time to intervene, which is sometimes as early as age five or six.
Will my child outgrow an underbite?
Severe underbites do not self-correct. While minor bite discrepancies sometimes improve as a child grows, a pronounced underbite where the lower jaw is significantly ahead of the upper jaw typically becomes more severe over time without intervention. The earlier we address an underbite, the more treatment options we have and the better the long-term stability of correction. Waiting to see if the child outgrows it usually means waiting until the problem is worse and correction is more complex.
Is appliance therapy uncomfortable for young children?
Most young children adapt to oral appliances very easily. There may be a brief adjustment period of a few days where the appliance feels new, but children typically acclimate quickly. Because the appliances we use work with natural growth rather than forcing movement, they don’t cause the discomfort associated with traditional braces. The appliance is worn during sleep, so it doesn’t interfere with daily activities. Parents are often surprised by how well their children comply with wearing the appliance once it becomes part of the bedtime routine.
How do I know if my child’s mouth breathing is serious enough to need treatment?
Any chronic mouth breathing should be evaluated. While occasional mouth breathing during colds or allergies is normal, a child who consistently breathes through their mouth, especially during sleep, likely has an underlying issue that should be addressed. Signs that mouth breathing is affecting your child include snoring, restless sleep, dark circles under the eyes, frequent waking, bedwetting, difficulty concentrating during the day, and chronic fatigue. Even without these symptoms, if your child’s mouth is consistently open rather than closed with lips together, an evaluation is worthwhile.
What happens if we decide to wait until my child is older to address an underbite?
Waiting until adolescence to address a significant underbite typically means the treatment will be more complex, invasive, and lengthy. Once facial growth is complete or nearly complete, the only way to correct a severe skeletal underbite is often orthognathic surgery combined with braces. This involves surgically repositioning the jaw bones, a procedure performed in a hospital under general anesthesia with a significant recovery period. By intervening early during the growth years, we can often correct the underbite non-surgically through growth guidance, avoiding the need for surgery entirely.
Will my child still need braces later if they have early intervention now?
Early intervention doesn’t necessarily eliminate the need for braces during adolescence, but it can significantly reduce the complexity and duration of later treatment. In some cases, children who receive early intervention may not need comprehensive braces at all, or may need only minor refinement. The primary goal of early intervention is to address skeletal issues, create adequate space for teeth, and establish proper jaw relationships. Fine-tuning tooth positions can be done more efficiently later if we’ve already established the proper foundation. Even when braces are still needed, the treatment is typically shorter and simpler than it would have been without early intervention.
Does early orthodontic treatment mean my child will be in treatment for a longer total time?
Not necessarily. Early intervention typically involves a phase of treatment during the primary or early mixed dentition, followed by a period of monitoring as permanent teeth erupt. If a second phase of treatment is needed during adolescence, it’s usually shorter than comprehensive treatment would have been without early intervention. The total time in active treatment may be similar or even less, and the treatment needed is less invasive. The key difference is that we’re working with growth during the early phase, accomplishing changes that would be impossible or require surgery if we waited.
What makes Central Park Dental & Orthodontics different from other practices?
At Central Park Dental & Orthodontics, we take a comprehensive approach that looks beyond teeth to consider facial development, airway function, and overall health. Our use of advanced diagnostic technology including three-dimensional CBCT imaging and specialized medical imaging visualization and analysis software allows us to identify and address issues that might be missed elsewhere. Dr. Jiyoung Jung has pursued extensive training in pediatric airway and development, bringing expertise that has been recognized through media features on NBC, ABC, FOX, CBS, and CW, and through consistent recognition as a D Magazine Best Dentist. We focus on early intervention when appropriate, working with natural growth to achieve optimal outcomes with the least invasive treatment possible.
Contact Central Park Dental & Orthodontics Today
If you’re concerned about your child’s bite, facial development, or breathing patterns, we invite you to schedule a comprehensive evaluation at Central Park Dental & Orthodontics. Located at 1101 Alexis Ct, Suite 101, Mansfield, TX 76063, we serve families throughout Mansfield, Arlington, Burleson, Alvarado, Grand Prairie, Kennedale, Lillian, Midlothian, and the greater Dallas-Fort Worth area.
Dr. Jiyoung Jung and our experienced team are committed to providing the highest level of care using advanced technology and evidence-based treatment approaches. We take the time to thoroughly evaluate each child, explain our findings, and discuss all available options so you can make informed decisions about your child’s care.
Early intervention can make a profound difference in your child’s development, comfort, and long-term health. The transformation shown in these before-and-after images represents what’s possible when we intervene at the optimal time with the right approach. Your child deserves the same opportunity for healthy development.
Call us today at 817-466-1200 to schedule a consultation. Let’s work together to give your child the foundation for a lifetime of healthy smiles, proper breathing, and optimal wellness. The earlier we address significant issues, the more we can accomplish with non-invasive treatment. Don’t wait and see—take action now to support your child’s best possible development.
Central Park Dental & Orthodontics is located at 1101 Alexis Ct #101, Mansfield, TX 76063. Dr. Jiyoung Jung and our team proudly serve patients from Mansfield, Arlington, Burleson, Alvarado, Dallas, Fort Worth, Grand Prairie, Kennedale, Lillian, and Midlothian. We are committed to providing comprehensive, airway-focused orthodontic care that supports whole-body wellness. Call 817-466-1200 to schedule your consultation today.
Related links:


